The passage introduces intestine-specific gene transfer (iGT), a method for delivering small molecules like siRNAs and plasmids into the intestinal epithelium of living mice using the Hemagglutinating Virus of Japan Envelope (HVJ-E). This technique offers a faster and more efficient alternative to traditional genetic engineering in mice, aiding research on intestinal stem cell-driven tissue renewal and tumorigenesis.
Key words: Intestinal epithelium, Hemagglutinating virus of Japan envelope (HVJ-E), Intestine specific gene transfer (iGT), Self-renewal
Introduction
This passage discusses the importance of stem cell-driven tissue renewal in multicellular organisms, with a focus on the intestinal epithelium. Intestinal stem cells (ISCs), located at the base of crypts, generate progenitor cells that continuously proliferate to maintain tissue renewal. These progenitors undergo differentiation into various intestinal cell types, such as enterocytes and goblet cells. While genetic studies in mice have been pivotal in understanding the signaling pathways (Wnt, Notch, BMP, Hedgehog) involved in intestinal homeostasis and tumorigenesis, mouse genetics is labor-intensive and time-consuming. To address these limitations, the authors developed a novel in vivo method called intestine-specific gene transfer (iGT). This method uses HVJ-E-based transfection to deliver small molecules like siRNAs and plasmids into the intestinal epithelium by fusing the viral envelope with the cell membrane. iGT allows efficient and transient gene transfer, providing a powerful tool for studying gene function in intestinal tissue renewal. The chapter includes a detailed protocol for iGT, technical notes, and methods for evaluating transfection efficiency.
Materials
Reagents and Solutions
1. Isoflurane.
2. Phosphate buffered saline (PBS).
3. GenomeONE-Si (for transfer of siRNA).
4. GenomeONE-Neo (for transfer of plasmids).
5. Cy3-labeled siRNA.
6. Mucus-removing solution: 20 mM dithiothreitol, 0.05% Tween 20 in PBS.
7. Nylon string.
8. 1 mLsyringe and 29-gauge needle.
9. 4% paraformaldehyde in PBS.
10. 12, 15, and 18% sucrose in PBS.
11. O.C.T. compound.
12. Cryomold.
13. Hoechst 33342.
14. Microscope slide.
15. Microcentrifuge tube.
16. 70% ethanol.
17. Mowiol.
Equipment
1. Small animal anesthetizer.
2. Surgical instruments (dissecting scissors, forceps, and surgical suture (4-0 nylon)).
3. Illuminated magnifier or surgical loupe.
4. Refrigerated microcentrifuge (for microtubes).
5. Cryostat microtome.
6. Epifluorescence microscope equipped with filters and illuminators suitable for observation of Cy3 fluorescence
Methods
Preparation of Transfection Solution
The following protocol is for transection of siRNAs into the intestinal epithelium by using GenomeONE-Si transfection reagent that
contains buffer solution, reagents D and E, and freeze-dried HVJ-E.
1. Add 260 μL of buffer solution to freeze-dried HVJ-E, mix gently but thoroughly by pipetting up and down, and then aliquot 120 μL of the HVJ-E solution into a 1.5 mL microcentrifuge tube.
2. Add 24μLofthe reagent D to the HVJ-E solution and mix by gently tapping the tube.
3. Centrifuge the tube at 10,000 g for 10 min at 4 C. After centrifugation, aspirate the supernatant and resuspend the pel let in 45 μLof20μM Cy3- labeled siRNA solution. Place the tube on ice until just before the injection into the mouse intestine.
4. Add 175 μL of buffer solution and 80 μL of the reagent E and mix by tapping the tube (see Note 1). Inject the solution into the mouse intestinal lumen according to the procedures described below (Subheading 3.2).
Preparation of Plasmid Transfection Solution (Optional)
For the transfection of plasmids into the intestinal epithelium, we used a GenomeONE-Neo transfection reagent containing
reagents A, B, and C, buffer solution, and HVJ-E solution.
1. Aliquot 120 μL of the HVJ-E solution into a 1.5 mL microcentrifuge tube. Add 30 μL of the reagent A to the solution,mix by tapping the tube, and incubate on ice for 5 min.
2. After incubation, add 30 μL of plasmids (1–2 μg/μL) and18 μL of the reagent B to the HVJ-E solution, and mix well by tapping the tube.
3. Centrifuge the tube at 10,000 g for 10 min at 4 C. After centrifugation, aspirate the supernatant, resuspend the pellet in 260 μL of buffer solution, and mix gently but thoroughly by pipetting up and down. Place the tube on ice until just before the injection into the mouse intestine.
4. Add 40 μL of the reagent C and mix by tapping the tube (see Note 1). Inject the solution into the mouse intestinal lumen.

Surgical Procedures for In Vivo Gene Transfer to the Mouse Intestinal Epithelium
1. Anesthetize mice with isoflurane. Mice should be fasted overnight to empty the proximal half of the small intestine. The abdomen is shaved and wiped with 70% ethanol. All surgical instruments are also disinfected with 70% ethanol.
2. Make an abdominal midline incision and blunt-dissect the skin from the peritoneum. Cut the peritoneum along the midline to address the small intestine.
3. Exteriorize a portion (about 5 cm long) of the small intestine, and gently suture (bind) its proximal and distal sides with nylon strings to seclude from the outer portion of the intestinal tract (Fig. 1). Use illuminated magnifier during suturing to avoid large blood vessels, as suturing can easily damage the blood vessels and cause bleeding (see Note 2). We usually wrap the mouseabdomenwithplastic films to avoid direct contact of the
intestinal tract with the mouse skin and hairs.
4. Fully distend the intestine by injecting 250–400 μL of mucus removing solution into the secluded region of the intestine with a 29-gauge needle syringe. Keep the distended state for 15 min.
5. Aspirate and inject the solution several times by a 29-gauge needle syringe to remove the mucus from the intestinal lumen, and then remove the solution as completely as possible.
6. Repeat steps 4 and 5.
7. Wash the same region of the intestine by injecting and aspirating PBSseveral times. Repeat this wash step at least three times.
8. Inject 250–400 μL of the siRNA transfection solution or plasmid transfection solution (see Subheading 3.1) into the intestinal lumen. The tissue should be fully distended at this time (see Note 3). Leave the mouse in this state for 1 h.
9. Unfasten the nylon strings at the proximal and distal ends of the injected region. Place the intestine back in the peritoneal cavity, close the skin with wound clips, and recover the mouse from anesthesia.
Dissection, Fixation,and Observation of the Transfected Tissue
1. 3 h after in vivo gene transfer (see Note 4), dissect the mouse and remove the injected region of the small intestine. Flush the intestinal lumen with cold PBS several times, and then fix the tissue for 1 h in 4% paraformaldehyde/PBS at 4 C with gentle agitation. Avoid the exposure to light throughout the following procedures to prevent quenching of Cy3 fluorescence.
2. After fixation, discard the fixative and wash the tissue with cold PBS three times for 10 min each.
3. Discard PBS and incubate the tissue in 12% sucrose/PBS for 2 hat 4 Cwithgentle agitation. After incubation, discard the solution and incubate the tissue sequentially in 15 and 18% sucrose/PBS for 2 h each.
4. After incubation in 18% sucrose/PBS, embed and freeze the tissue in O.C.T Compound.
5. Cut 4–8 μmsections of the frozen intestinal specimen by using a cryostat microtome and mount the sections onto a microscope slide. Allow sections to air dry for a few minutes.
6. Wash sections in PBS for 5 min to remove O.C.T. Compound. To stain the nuclei of cells, incubate the sections with Hoechst 33342 diluted in PBS (1/500–1000) for 10 min at room temperature.
7. Aspirate Hoechst 33342 and wash sections in PBS three times for 5 min each. Rinse the slide briefly in DDW, and then seal the sections with the Mowiol mounting medium and coverslips.
8. Observe Cy3 and Hoechst 33342 fluorescence on the tissuesections with an epifluorescence microscope (see Note 5)
Notes
1. After addition of the reagents C and E, HVJ-E particles are sticky and can easily form large aggregates in the solution. For
the efficient transfection, the reagent C and E should be added immediately before the injection of transfection solution.
2. Intestinal injury can cause the formation of fibrous bands(adhesions) in the abdomen, which induces severe life threatening intestinal obstruction. To reduce the risk for intestinal obstruction, it is critical to minimize injury and bleeding during the iGT procedures. Especially, care should be taken to avoid damaging visible blood vessels when binding the intestinal tract with nylon strings and injecting solution into the lumen.
3. Insufficient distention of the intestinal tract during iGT results in inefficient transfection into the crypt compartment. Even in such cases, the villus compartments are usually transfected with high efficiency. Since crypts are hidden between and below the villi, distention of the tract is required to expose them to the transfection solution.
4. HVJ-E-mediated transfer of the incorporated molecules into the intestinal epithelium is achieved within a few hours. For the observation of fluorescently labeled siRNAs, it is better to observe the transfected tissue within 3–5 h, as fluorescence would be gradually decreased thereafter. However, it should be important to keep in mind that the knockdown of target genes by siRNAs and expression of transgenes from plasmids would take more time (typically 2–3 days) and last for up to 5–7 days after transfection. Thus, the effects of transfection on the tissue phenotypes should be analyzed during this period.
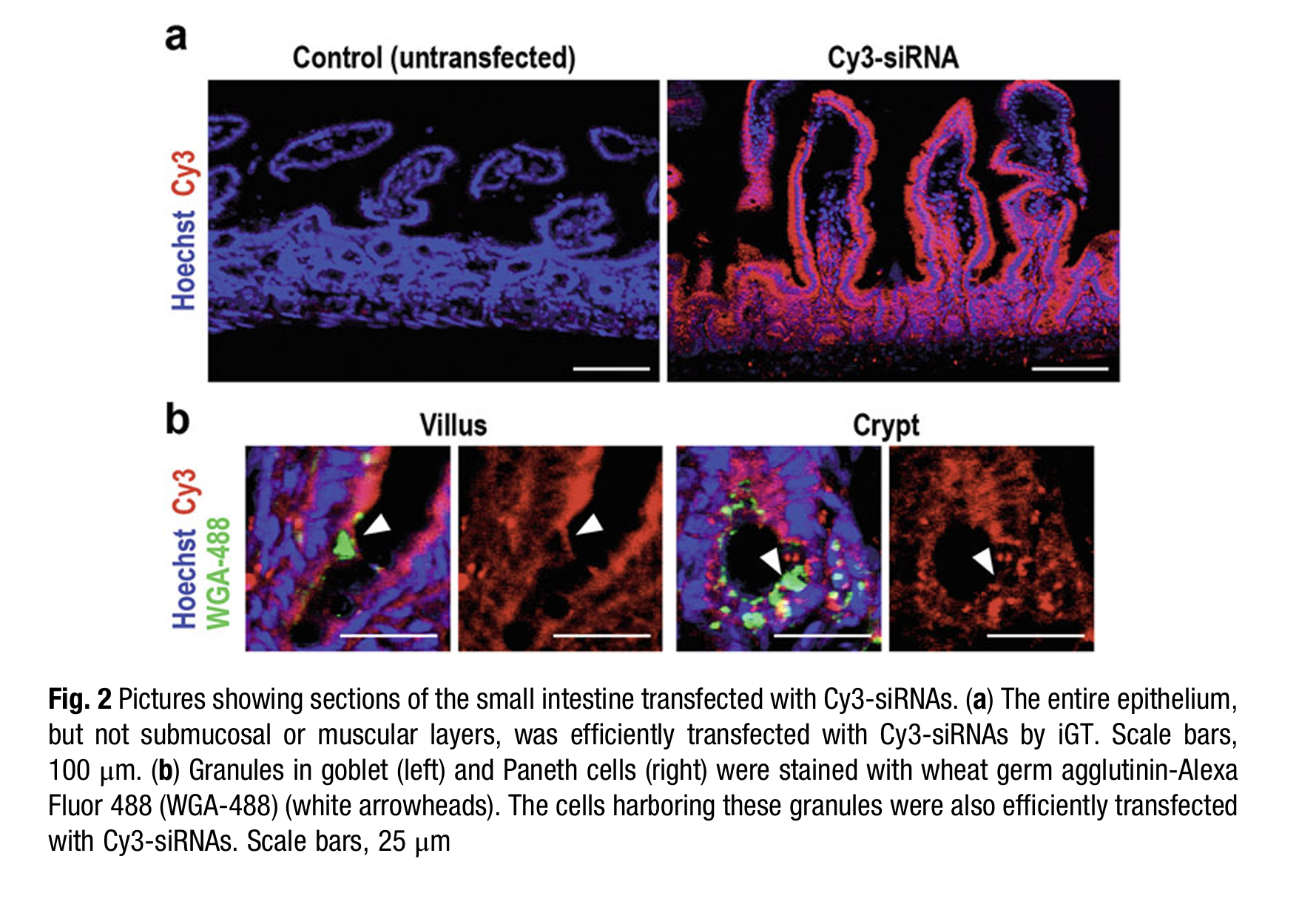
5. The typical results of transfection of Cy3-labeled siRNAs are shown in Fig. 2. Cy3 fluorescence could be observed from immediately after transfection in the entire epithelium including both villus and crypt compartments (Fig. 2a). By contrast,the submucosal layer or smooth muscle layer does not emit fluorescence, indicating that iGT transfers incorporated molecules specifically into the epithelium. By costaining granules in
goblet and Paneth cells with Alexa Fluor 488-labeled lectin (wheat germ agglutinin (WGA)), one could confirm that the two types of cells are efficiently transfected with Cy3-labeled siRNAs (Fig. 2b). The other types of epithelial cells, including intestinal stem cells, progenitor cells, enterocytes, and enteroendocrine cells, could be also transfected by iGT.




